Introduction: Endoscopic internal urethrotomy is the standard surgical treatment for short strictures of the male urethra. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures. Materials and methods: This was a retrospective, cross-sectional descriptive study conducted in the urology department of the Pr Bocar Sidy Sall University Hospital in Kati over a 36-month period from January 1, 2022, to December 31, 2024. Results: We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range from 16 to 90 years. The most frequent symptom was dysuria and pollakiuria, with a frequency of 42.5%. The diagnosis was confirmed in 75% of cases by UCR-M. The length of the strictures was 2 cm or less in 90% of cases. The stricture was located in the bulb of the urethra in 42.5% of cases. The etiology was predominantly iatrogenic in 52.5% of cases, followed by post-traumatic strictures in 22.5%. The average length of hospital stay was 3 days. The outcome was satisfactory in 87.5% of cases. Conclusion: Endoscopic internal urethrotomy is the standard treatment for short urethral strictures. It provides good functional and anatomical results.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Endoscopic internal urethrotomy consists of an endoscopic incision of the stricture under direct visual control, in order to restore the urethral caliber. It has become established as a minimally invasive, relatively simple, reproducible, and accessible technique in facilities equipped with adequate endoscopic equipment. It is indicated for strictures of the short urethra. Numerous techniques have been proposed for treating male urethral strictures over the years. Among these techniques is endoscopic internal urethrotomy, first described by Maisonneuve and Otis
[1]
Otis FN. Remarks on strictures of urethrae of extreme calibre, with cases and description of new instrument for their treatment. N. Y. Med. J. 1972; 15: 152.
[1]
, who performed it blindly, and then by Saches
[2]
Sachse H. Transurethral sharp sclerotherapy of the urethral stricture with a visual urethrotum. Verh Dt. Ges. Urol., 1973, 25, 143.
[2]
, who was the first, in 1973, to develop the method under direct visual control. The treatment of urethral strictures includes various techniques, such as dilation, endoscopic internal urethrotomy, and urethroplasty. Currently, endoscopic internal urethrotomy (EIU) is the first-line treatment for urethral stricture for most authors
[3]
Benjelloun M, Drissi M, Makhloufi M, Nouri A, Karmouni T, Tazi K et al. Treatment of urethral strictures by endoscopic internal urethrotomy: anatomical and functional results of a series of 244 cases. Africain Journal of Urology 2008; 14 (2): 114-119.
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[3, 4]
. Endoscopic internal urethrotomy involves an endoscopic incision of the stricture under direct visual control to restore the urethral caliber. It has become established as a minimally invasive, relatively simple, reproducible, and readily available technique in facilities equipped with appropriate endoscopic equipment. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures.
2. Materials and Methods
Study Setting:
The study was conducted in the Urology Department of the Professor Bocar Sidy Sall University Hospital Center in Kati.
Study Type:
This was a retrospective, cross-sectional descriptive study.
Study Period:
Our study took place over a 3-year period, from January 1, 2022, to December 31, 2024.
Study Population:
Our study population included all male patients, regardless of origin, marital status, or age, admitted to the Urology Department of the Professor Bocar Sidy Sall University Hospital Center in Kati who underwent an endoscopic internal urethrotomy (EIU) during the study period. Sampling:
Inclusion criteria:
All patients who underwent endoscopic internal urethrotomy (EIU) for male urethral stricture at the urology department of the Pr BSS University Hospital in Kati during the study period and who had a complete medical record were included.
Materials:
We used a Storz CH 21 urethrotome, a 30° optic, a light source, and an endoscopy video tower. The passive trigger used was also Storz.
Data sources:
The data sources for our study were: operative reports, hospitalization records, and medical records (consultations and hospitalizations).
Data collection and analysis:
Data were collected using a questionnaire. The questionnaires were entered and analyzed using Word 2019, Excel 2016, and SPSS version 22.0 after data verification. Ethical and professional considerations: Informed consent was obtained from all patients before their inclusion in the study.
The information provided by each patient was completely confidential and used solely for research purposes. Each patient's personal information was coded with a number that prevented identification of the individual upon publication of the study results.
3. Results
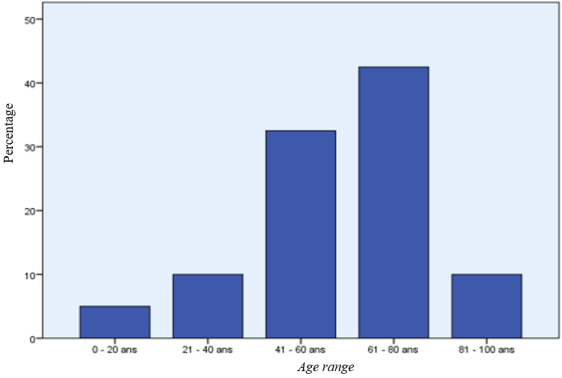
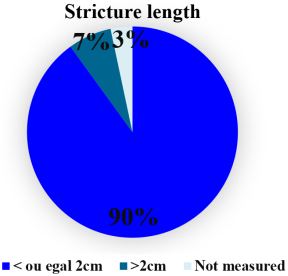
We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. Endoscopic surgery was performed in 646 patients, accounting for 80.0% of our procedures. The mean age of our patients was 45.3 years, with a range from 16 to 90 years (Figure 1). The most frequent symptom was the combination of dysuria and pollakiuria, with a frequency of 42.5% (Table 1). E. coli was the most frequently isolated pathogen, at 68.2% (Table 2). The diagnosis was confirmed in 75% of cases by urinary urethrotomy. The length of the strictures was less than or equal to 2 cm in 90% of cases (Figure 2). The stricture was located in the bulb of the urethra in 42.5% of cases (Table 3). The etiology was predominantly iatrogenic strictures in 52.5% of cases, followed by post-traumatic strictures in 22.5% (Table 4). Simple endoscopic internal urethrotomy (EIU) was performed in 47.5% of cases (Table 5). The average length of hospital stay was 3 days (Table 6). Removal of the transurethral bladder catheter was performed in 25 of our patients within 0-7 days, representing a rate of 62.5% (Table 7). The outcome was satisfactory in 87.5% of cases (Table 8).
Figure 2. Distribution of patients according to the size of the urethral stricture. Urethral stricture was < or equal to 2 cm in 90% of cases.
Table 1. Distribution of patients according to symptomatology.
Symptomatology
Effective
Percentage (%)
Dysuria + Pollakiuria
17
42.5
Dysuria + Pollakiuria + burning during urination
13
32.5
Urethrorrhagia
5
12.5
Hematuria
3
7.5
Simple Dysuria
2
5.0
Total
40
100
Dysuria + pollakiuria was the most common symptom in our study series.
Table 2. Distribution of patients according to the germ found in the urine culture.
Germ
Effective
Percentage (%)
E. Coli
15
68.2
Klebsiella Pneumoniae
4
18.2
Neisseria Gonorrhoeae
2
9.1
Staphylococcus Aureus
1
4.5
Total
22
100
E. coli was the most frequently found germ, at a rate of 68.2%.
Table 3. Distribution of patients according to the location of urethral stricture.
Location
Effective
Percentage (%)
Bulbar
18
45.0
Membranous
10
25.0
Bulbo-membranous
9
22.5
Penile
3
7.5
Total
40
100
The bulbar portion was the most frequently found location, at 45%.
Table 4. Distribution of patients according to the etiology of urethral stricture.
Etiology
Effective
Percentage (%)
Iatrogenic
21
52.5
Post-traumatic
9
22.5
Infectious
7
15.0
Tumoral
3
10.0
Total
40
100
Iatrogenic urethral stricture accounted for 52.5% of cases.
Table 5. Distribution of patients according to the type of intervention.
Type of intervention
Effective
Percentage (%)
Simple EIU
19
47.5
EIU + TRUP
7
17.5
EIU + cervicoprostatic incision
6
15.0
EIU + TURB + hydrocele treatment
2
5.0
EIU + TRUB
1
2.5
EIU + intravesical lithotripsy
1
2.5
EIU + inguinal hernia repair
1
2.5
EIU + cystolithotomy
1
2.5
EIU + TURP + cystolithotomy
1
2.5
EIU + scrototomy
1
2.5
Total
40
100
Simple EIU was performed in 47.5% of cases.
Table 6. Distribution of patients according to length of hospital stay in days.
Length of hospital stay in days
Effective
Percentage (%)
3 days
18
45.0
2 days
15
37.5
4 days
3
7.5
6 days
3
7.5
5 days
1
2.5
Total
40
100
The length of hospital stay was 3 days for 18 of our patients, or 45%.
Table 7. Distribution of patients according to the time ejection of the probe.
Time frame for removal of the transurethral bladder catheter
Effective
Percentage %
0-7
25
62.5
8-14
7
17.5
15-21
6
15.0
22-28
2
5.0
Total
40
100
Removal of the transurethral bladder catheter was performed in 25 of our patients within a 0-7 day interval, representing a rate of 62.5%.
Table 8. Distribution of patients according to the result of the postoperative urinary status.
Postoperative urinary status
Effective
Percentage (%)
Good
35
87.5
Average
3
7.5
Poor
2
5.0
Total
40
100
Post-operative urinary status was good in 35 cases, or 87.5%.
4. Discussion
We performed 40 cases of endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range of 16 to 90 years. This mean age is similar to that of the study by MS Ousman Manzo
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
, which was 50.82 years, with a range of 17 to 82 years. The main symptom of urethral stricture is dysuria. The most frequent symptom was the combination of dysuria and pollakiuria, with a frequency of 42.5%. Dysuria was the most common reason for consultation.
The main reason for consultation was also dysuria in the studies of several authors, specifically 55.79% in the study by Avion et al.
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[4]
and 54.4% in that of MS Ousman Manzo et al.
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
Diarra A. Anatomical and functional results of endoscopic internal urethrotomy in the urology department of the CHU-ME Luxembourg. Medical thesis; Bamako, 2023, n°31, 108p.
[6]
which represented 40% and was lower than Kassogue. A et al.
[7]
Kassogue A, Diarra A, Diallo M, Diarra M, Sissoko I, Sangare D. Etiologies and management of urethral stricture in Kati (Mali). Health Res Afr 2025; 3: 24-8.
[7]
which represented 80.6%.
E. coli was the most frequently detected organism in our study, at a rate of 68.2%. Urinary tract infection complicates the clinical picture and exacerbates urinary symptoms. Urological history was dominated by urinary tract infection, with 33 cases, or 57.9% (n=31)
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
The diagnosis was confirmed in 75% of cases by retrograde and voiding urethrocystography (RVUC), which is the gold standard for diagnosing urethral stricture. The length of the strictures was less than or equal to 2 cm in 90% of cases. The most common location of the stricture was the bulb, at 38.6% in our study; this bulbar location was higher in the study by Avion et al., at 42.5%
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[4]
. The etiology was dominated by iatrogenic strictures in 52.5%, followed by post-traumatic strictures in 22.5% (Table 4). In contrast, the etiologies were infectious in 51.50% and traumatic in 32.18%, according to the results of Avion et al.
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[4]
. Simple EIU was performed in 47.5% of cases without any other endoscopic procedures. In the study by MS Ousman Manzo et al.
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
, simple EIU was the most common procedure, occurring in 57.9% of cases.
The average length of hospital stay was 3 days (Table 6). This is similar to the study by MS Ousman Manzo
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
, where the average length of stay was 4.5 days with a favorable outcome in 94.7% of cases. This average postoperative length of stay was higher in the study by Dje K et al., at 6.8 days, with a range of 0 to 38 days
[8]
Dje K, Coulibaly A, Coulibaly N, Sangare IS. Endoscopic internal urethrotomy in the treatment of acquired urethral stricture in black Africans: a study of 140 cases. Medecine d'Afrique Noire 1999; 46 (1): 56-61.
[8]
.
Removal of the transurethral bladder catheter was performed in 25 of our patients within a range of 0 to 7 days, representing a rate of 62.5%. This catheterization duration was ≥ 5 days in 45.4% of patients in the study by S. Zouari
[9]
Zouari S, Saadi A, Setti Boubaker N, Said R, Zaghbib S, Hermi A et al. Impact of catheterization duration, catheter type and diameter on urethral stricture recurrence after endoscopic internal urethrotomy. Prog. Urol. 2024: 105-106.
[9]
. Benjelloun et al.
[3]
Benjelloun M, Drissi M, Makhloufi M, Nouri A, Karmouni T, Tazi K et al. Treatment of urethral strictures by endoscopic internal urethrotomy: anatomical and functional results of a series of 244 cases. Africain Journal of Urology 2008; 14 (2): 114-119.
[3]
reported an average duration of postoperative catheterization of 2 days and that maintaining catheterization beyond this time did not provide significant improvement. However, the average duration of postoperative urinary catheterization was 14 days
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[4]
. S. Zouari
[9]
Zouari S, Saadi A, Setti Boubaker N, Said R, Zaghbib S, Hermi A et al. Impact of catheterization duration, catheter type and diameter on urethral stricture recurrence after endoscopic internal urethrotomy. Prog. Urol. 2024: 105-106.
[9]
reports that reducing the duration of postoperative catheterization, using silicone catheters, and increasing the catheter gauge could improve the success rate of endoscopic internal urethrotomy (EIU), but that further prospective randomized studies are needed to confirm these results. Endoscopic internal urethrotomy is a simple, repeatable technique with straightforward postoperative recovery and a shorter hospital stay
[8]
Dje K, Coulibaly A, Coulibaly N, Sangare IS. Endoscopic internal urethrotomy in the treatment of acquired urethral stricture in black Africans: a study of 140 cases. Medecine d'Afrique Noire 1999; 46 (1): 56-61.
[8]
.
The outcome was satisfactory in 87.5% of cases. A stable success rate of approximately 75.4% at 3.5 years was observed in de Benjelloun et al.
[3]
Benjelloun M, Drissi M, Makhloufi M, Nouri A, Karmouni T, Tazi K et al. Treatment of urethral strictures by endoscopic internal urethrotomy: anatomical and functional results of a series of 244 cases. Africain Journal of Urology 2008; 14 (2): 114-119.
[3]
. EIU can be offered as a first-line treatment for any short, single urethral stricture of the posterior urethra. This result was even better when the procedure involved a short (less than 2 cm), single stricture of the posterior urethra
[3]
Benjelloun M, Drissi M, Makhloufi M, Nouri A, Karmouni T, Tazi K et al. Treatment of urethral strictures by endoscopic internal urethrotomy: anatomical and functional results of a series of 244 cases. Africain Journal of Urology 2008; 14 (2): 114-119.
[3]
. Endoscopic internal urethrotomy (EIU) is a technique applicable to short, single, and 1-cm strictures of the posterior urethra that can be traversed with a blade, Ngaroua et al.
[10]
Ngaroua N, Eloundou NJ, Djibrilla Y, Asmaou O, Mbo AJ. Epidemiological, clinical aspects and management of urethral stenosis in adult patients in a District Hospital in Ngaoundéré, Cameroon. Pan Afr Med J 2017; 26: 1-6.
. It produces satisfactory results for strictures up to two centimeters in length
[10]
Ngaroua N, Eloundou NJ, Djibrilla Y, Asmaou O, Mbo AJ. Epidemiological, clinical aspects and management of urethral stenosis in adult patients in a District Hospital in Ngaoundéré, Cameroon. Pan Afr Med J 2017; 26: 1-6.
In our study, the outcome was satisfactory in 87.5% of cases. Postoperative outcomes were favorable, with a 62.50% success rate (25 cases) and a 17.50% recurrence rate (7 cases). Niang et al.
[11]
Niang L. Results of endoscopic internal urethrotomy at the urology and andrology department of Aristide Le Dantec Hospital: a study of 61 cases. Medical thesis. Dakar, 2003, n°09, 82p.
[11]
reported a 70% success rate. There was no intraoperative or postoperative mortality. Endoscopic internal urethrotomy is currently the gold standard for the surgical management of short strictures of the posterior urethra.
5. Conclusion
Endoscopic internal urethrotomy is the standard surgical treatment for short urethral strictures. The procedure is simple and quick, with no major morbidity and requiring only a short hospital stay. It reduces the duration of bladder catheterization after the procedure. The functional outcome is satisfactory.
Abbreviations
CHU
University Hospital Center
BSS
Bocar Sidy Sall
USTTB
University of Sciences, Techniques and Technologies of Bamako
Otis FN. Remarks on strictures of urethrae of extreme calibre, with cases and description of new instrument for their treatment. N. Y. Med. J. 1972; 15: 152.
[2]
Sachse H. Transurethral sharp sclerotherapy of the urethral stricture with a visual urethrotum. Verh Dt. Ges. Urol., 1973, 25, 143.
[3]
Benjelloun M, Drissi M, Makhloufi M, Nouri A, Karmouni T, Tazi K et al. Treatment of urethral strictures by endoscopic internal urethrotomy: anatomical and functional results of a series of 244 cases. Africain Journal of Urology 2008; 14 (2): 114-119.
[4]
Avion KP, N’Diamoi A, Ouattara F, Aguia B, Zouan F, Alloka V et al. Endoscopic Internal Urethrotomy (EIU) for the Treatment of Ureteral Stenosis: A Review of 233 Cases. Open Journal of Urology, 2021, 11, 264-272.
[5]
Ousman Manzo MS, Karimoune Mossi O, Boka Tounga Y, Seydou Hamadou A, Adamou Kaka MS, Dambaki Maman S, Soumana A. The role of endoscopic internal urethrotomy in the treatment of urethral stricture. Jaccr Africa 2024; 8(3): 268-276.
Diarra A. Anatomical and functional results of endoscopic internal urethrotomy in the urology department of the CHU-ME Luxembourg. Medical thesis; Bamako, 2023, n°31, 108p.
[7]
Kassogue A, Diarra A, Diallo M, Diarra M, Sissoko I, Sangare D. Etiologies and management of urethral stricture in Kati (Mali). Health Res Afr 2025; 3: 24-8.
[8]
Dje K, Coulibaly A, Coulibaly N, Sangare IS. Endoscopic internal urethrotomy in the treatment of acquired urethral stricture in black Africans: a study of 140 cases. Medecine d'Afrique Noire 1999; 46 (1): 56-61.
[9]
Zouari S, Saadi A, Setti Boubaker N, Said R, Zaghbib S, Hermi A et al. Impact of catheterization duration, catheter type and diameter on urethral stricture recurrence after endoscopic internal urethrotomy. Prog. Urol. 2024: 105-106.
[10]
Ngaroua N, Eloundou NJ, Djibrilla Y, Asmaou O, Mbo AJ. Epidemiological, clinical aspects and management of urethral stenosis in adult patients in a District Hospital in Ngaoundéré, Cameroon. Pan Afr Med J 2017; 26: 1-6.
Niang L. Results of endoscopic internal urethrotomy at the urology and andrology department of Aristide Le Dantec Hospital: a study of 61 cases. Medical thesis. Dakar, 2003, n°09, 82p.
Kassogue, A., Traore, B., Sylla, H., Tolo, S., Sissoko, I., et al. (2026). Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. International Journal of Clinical Urology, 10(1), 65-70. https://doi.org/10.11648/j.ijcu.20261001.22
Kassogue, A.; Traore, B.; Sylla, H.; Tolo, S.; Sissoko, I., et al. Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. Int. J. Clin. Urol.2026, 10(1), 65-70. doi: 10.11648/j.ijcu.20261001.22
Kassogue A, Traore B, Sylla H, Tolo S, Sissoko I, et al. Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. Int J Clin Urol. 2026;10(1):65-70. doi: 10.11648/j.ijcu.20261001.22
@article{10.11648/j.ijcu.20261001.22,
author = {Amadou Kassogue and Boubacar Traore and Hamed Sylla and Saydou Tolo and Idrissa Sissoko and Daouda Sangare and Issa Coulibaly and Moussa Salifou Diallo and Mamadou Lamine Diakite},
title = {Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {65-70},
doi = {10.11648/j.ijcu.20261001.22},
url = {https://doi.org/10.11648/j.ijcu.20261001.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.22},
abstract = {Introduction: Endoscopic internal urethrotomy is the standard surgical treatment for short strictures of the male urethra. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures. Materials and methods: This was a retrospective, cross-sectional descriptive study conducted in the urology department of the Pr Bocar Sidy Sall University Hospital in Kati over a 36-month period from January 1, 2022, to December 31, 2024. Results: We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range from 16 to 90 years. The most frequent symptom was dysuria and pollakiuria, with a frequency of 42.5%. The diagnosis was confirmed in 75% of cases by UCR-M. The length of the strictures was 2 cm or less in 90% of cases. The stricture was located in the bulb of the urethra in 42.5% of cases. The etiology was predominantly iatrogenic in 52.5% of cases, followed by post-traumatic strictures in 22.5%. The average length of hospital stay was 3 days. The outcome was satisfactory in 87.5% of cases. Conclusion: Endoscopic internal urethrotomy is the standard treatment for short urethral strictures. It provides good functional and anatomical results.},
year = {2026}
}
TY - JOUR
T1 - Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures
AU - Amadou Kassogue
AU - Boubacar Traore
AU - Hamed Sylla
AU - Saydou Tolo
AU - Idrissa Sissoko
AU - Daouda Sangare
AU - Issa Coulibaly
AU - Moussa Salifou Diallo
AU - Mamadou Lamine Diakite
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.22
DO - 10.11648/j.ijcu.20261001.22
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 65
EP - 70
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.22
AB - Introduction: Endoscopic internal urethrotomy is the standard surgical treatment for short strictures of the male urethra. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures. Materials and methods: This was a retrospective, cross-sectional descriptive study conducted in the urology department of the Pr Bocar Sidy Sall University Hospital in Kati over a 36-month period from January 1, 2022, to December 31, 2024. Results: We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range from 16 to 90 years. The most frequent symptom was dysuria and pollakiuria, with a frequency of 42.5%. The diagnosis was confirmed in 75% of cases by UCR-M. The length of the strictures was 2 cm or less in 90% of cases. The stricture was located in the bulb of the urethra in 42.5% of cases. The etiology was predominantly iatrogenic in 52.5% of cases, followed by post-traumatic strictures in 22.5%. The average length of hospital stay was 3 days. The outcome was satisfactory in 87.5% of cases. Conclusion: Endoscopic internal urethrotomy is the standard treatment for short urethral strictures. It provides good functional and anatomical results.
VL - 10
IS - 1
ER -
Kassogue, A., Traore, B., Sylla, H., Tolo, S., Sissoko, I., et al. (2026). Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. International Journal of Clinical Urology, 10(1), 65-70. https://doi.org/10.11648/j.ijcu.20261001.22
Kassogue, A.; Traore, B.; Sylla, H.; Tolo, S.; Sissoko, I., et al. Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. Int. J. Clin. Urol.2026, 10(1), 65-70. doi: 10.11648/j.ijcu.20261001.22
Kassogue A, Traore B, Sylla H, Tolo S, Sissoko I, et al. Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures. Int J Clin Urol. 2026;10(1):65-70. doi: 10.11648/j.ijcu.20261001.22
@article{10.11648/j.ijcu.20261001.22,
author = {Amadou Kassogue and Boubacar Traore and Hamed Sylla and Saydou Tolo and Idrissa Sissoko and Daouda Sangare and Issa Coulibaly and Moussa Salifou Diallo and Mamadou Lamine Diakite},
title = {Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {65-70},
doi = {10.11648/j.ijcu.20261001.22},
url = {https://doi.org/10.11648/j.ijcu.20261001.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.22},
abstract = {Introduction: Endoscopic internal urethrotomy is the standard surgical treatment for short strictures of the male urethra. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures. Materials and methods: This was a retrospective, cross-sectional descriptive study conducted in the urology department of the Pr Bocar Sidy Sall University Hospital in Kati over a 36-month period from January 1, 2022, to December 31, 2024. Results: We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range from 16 to 90 years. The most frequent symptom was dysuria and pollakiuria, with a frequency of 42.5%. The diagnosis was confirmed in 75% of cases by UCR-M. The length of the strictures was 2 cm or less in 90% of cases. The stricture was located in the bulb of the urethra in 42.5% of cases. The etiology was predominantly iatrogenic in 52.5% of cases, followed by post-traumatic strictures in 22.5%. The average length of hospital stay was 3 days. The outcome was satisfactory in 87.5% of cases. Conclusion: Endoscopic internal urethrotomy is the standard treatment for short urethral strictures. It provides good functional and anatomical results.},
year = {2026}
}
TY - JOUR
T1 - Endoscopic Internal Urethrotomy in the Management of Male Urethral Strictures
AU - Amadou Kassogue
AU - Boubacar Traore
AU - Hamed Sylla
AU - Saydou Tolo
AU - Idrissa Sissoko
AU - Daouda Sangare
AU - Issa Coulibaly
AU - Moussa Salifou Diallo
AU - Mamadou Lamine Diakite
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.22
DO - 10.11648/j.ijcu.20261001.22
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 65
EP - 70
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.22
AB - Introduction: Endoscopic internal urethrotomy is the standard surgical treatment for short strictures of the male urethra. The objective was to evaluate the outcomes of endoscopic internal urethrotomy in the management of male urethral strictures. Materials and methods: This was a retrospective, cross-sectional descriptive study conducted in the urology department of the Pr Bocar Sidy Sall University Hospital in Kati over a 36-month period from January 1, 2022, to December 31, 2024. Results: We identified 40 patients who underwent endoscopic internal urethrotomy, representing a frequency of 6.2%. The mean age of our patients was 45.3 years, with a range from 16 to 90 years. The most frequent symptom was dysuria and pollakiuria, with a frequency of 42.5%. The diagnosis was confirmed in 75% of cases by UCR-M. The length of the strictures was 2 cm or less in 90% of cases. The stricture was located in the bulb of the urethra in 42.5% of cases. The etiology was predominantly iatrogenic in 52.5% of cases, followed by post-traumatic strictures in 22.5%. The average length of hospital stay was 3 days. The outcome was satisfactory in 87.5% of cases. Conclusion: Endoscopic internal urethrotomy is the standard treatment for short urethral strictures. It provides good functional and anatomical results.
VL - 10
IS - 1
ER -